How To Render First Aid. Continued
Description
This section is from "Every Woman's Encyclopaedia". Also available from Amazon: Every Woman's Encyclopaedia.
How To Render First Aid. Continued
7. Hysterics is most common among ill-controlled girls when passing into womanhood, and the condition shows a need for medical treatment. Crying and laughing alternate rapidly, and there is blinking at the eyes. Such fits never occur when a girl is alone, and when she is suffering from one she is on the qui vive to find out what treatment will be adopted. If of the kind and gentle order the fit continues, but drastic measures promote a sudden recovery. Show no sympathy, but apply strong ammonia to the nose, and dash cold water in the face. Or, better still, leave the room quickly, slam the door hind, and on no account return.
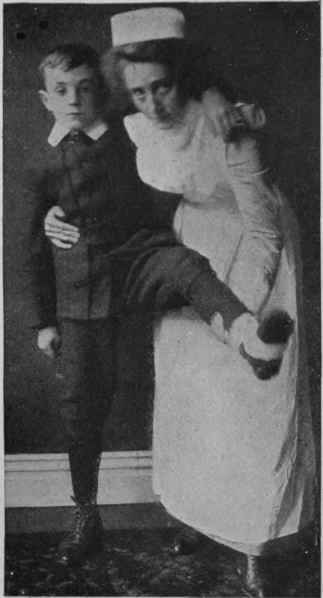
Fig. 2. Assisting a patient with an injured leg when only one helper is available
The General Treatment of Insensibility may be summed up as follows:
1. Arrange for a plentiful supply of fresh air.
2. Loosen all tight clothing, particularly round the neck.
3. Have the head slightly raised, excepting in fainting fits, when it should hang low.
4. Apply ice or cold water to the head, and heat to the other extremities.
Note. - In applying hot-water bottles or hot bricks see that they are wrapped in flannel, so as to avoid the risk of burning the patient.
5. Keep the room dark and cool.
6. Avoid giving liquids to an unconscious person, and particularly alcoholic beverages.
7. Seek medical aid.
The Transport of the Injured
In cases of injury or sudden illness it may be necessary to convey a patient from one place to another. The illustrations show so clearly certain simple methods of transporting the injured that detailed instructions are not necessary.
Fig. 2 shows how to assist a patient who has injured the leg when only one helper is available. The helper stands on the injured side of the patient, who places his arm around the helper's neck. The helper's arm which is nearer the patient passes behind his back, and then presses his hip, while the free hand is available for supporting the injured limb, which must be steadied while the patient hops forward.
Fig. 3 shows a two-handed seat, which is particularly serviceable to a weak patient, on account of its strong back support.

Fig. 3. A two-handed seat which affords a good back support when a patient is to be carried seat for a patient. This form of

Fig. 4. Forming a three-handed seat is firmer than a two-handed one
Fig. 4 shows a three-handed seat, which is firmer than the two-handed seat, yet has a fairly firm back support.
Fig. 5 shows the firmest of all seats, made by the union of four hands, each of which grasps the wrist nearest to it and towards the left as the two bearers stand facing each other with hands extended.
The patient clasps each bearer round the neck. Fig. 6 shows a useful carrying sheet, improvised by buttoning a coat or mackintosh down the front, and keeping it taut by two broom-handles or poles which pass down the sides and through the sleeves.
The patient sits between the poles, and leans his back against the back of the forward bearer.
Similarly, for a patient who has to be carried in a recumbent position, a stretcher can be improvised from two coats and two poles, or by rolling two poles one in each of the opposite sides of a tarpaulin until it is of a suitable width; or a hurdle, a shutter, a door, or a gate might be used as an improvised ambulance.
No patient should be placed on a stetcher until the necessary first aid treatment has been rendered - until bleeding has been controlled, and fractured limbs made perfectly rigid with splints.
In moving a patient on a stretcher, from two to four bearers are necessary, according to the weight of the patient and the distance to be travelled. Indeed, for carrying a heavy patient a long distance, relays of bearers are desirable. One of the number must be appointed captain to issue orders, so that all may work harmoniously together, and thus minimise the risk of jarring the patient.

Fig. 5. The four-handed seat. This is the firmest of seats, but affords no support for the back
The stretcher must be placed in position in line with the patient's body, and with the foot of it close to his head. Bearers 1 and 2 face each other on either side of the patient's body, and the captain and bearer 4 take similar position by his knees.
The captain takes charge of the injured limb or limbs, and sees that no bandages or splints are displaced, and at the time of lifting must place his hands underneath the lower limbs, taking care when dealing with a fracture to have one hand above, and another below the seat of injury.
Each bearer sinks on one knee and grasps the hands of his vis-a-vis under the patient. At the word of command the bearers rise, and march till the patient's head is over the pillow of the stretcher. Similarly, they each kneel on one knee to lower the patient on the stretcher, and when he is comfortably arranged and well covered, they raise the stretcher and march at the word of command from the captain, who acts as hind bearer so as to keep a careful watch on the patient.
The step for marching must be short, with movement of the knee-joint rather than the hips.
Unload ing the stretcher is similarly performed, with the bearers kneeling on one knee.
The sleeves

Fig. 6. A carrying sheet, improvised by buttoning a coat down the front. It is kept taut by broonvhandles that pass down the sides and through
Continue to:
My Books

