Anteversion
Description
This section is from the book "Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs", by Percy H. Woodall, M. D., D.O.. Also available from Amazon: Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs.
Anteversion
This is a condition in which the uterus is rigid and the cervico-corporeal angle is either normal or extended, the fundus is turned forward and downward and the cervix passes upward and backward. The normal flexion and flexibility of the uterus is lost and the cervix and the body form one rigid whole (Fig. 23).
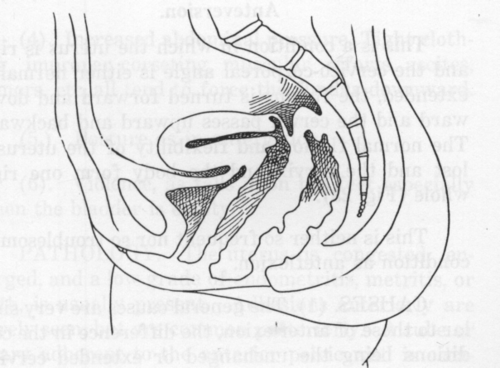
Fig. 23. Anteversion.
This is neither so frequent nor so troublesome a condition as anteflexion.
Causes
(1). The general causes are very similar to those of anteflexion, the difference in the conditions being the unchanged or extended cervico-corporeal angle and the rigidity of the tissue at this point in anteversion. Disturbed spinal innervation operates as in anteflexion.
(2.) Chronic congestion, endometritis, subinvolution, tumors, pregnancy, etc. All of these conditions increase the weight of the uterus and cause it to tip forward when the individual is sitting or standing.
(3). Inflammatory Adhesions. These may rarely be in the anterior portion of the pelvis and draw the fundus forward and downward. More frequently they are along the course of the sacro-uterine ligaments, and draw the cervix upward. The cervico-corporeal angle being rigid, the fundus of necessity tips forward.
(4). Increased abdominal pressure. Tight clothing, improper corseting, muscular efforts, ascites, tumors, etc, all tend to force the fundus downward.
(5.) Posture as in anteflexion.
(6). Violence, as falls upon the feet especially when the bladder is empty.
Pathology
The uterus is congested, enlarged, and a low grade of endometritis, metritis, or both, is usually present. Adhesions anteriorly are rarely seen, but are common posteriorly. A tube or ovary adherent to the anterior pelvic wall is occasionally found.
When not involved in adhesions the sacro-uterine ligaments are retracted from non-use. Some degree of cystitis may be present.
Symptoms
These are not as pronounced and constant as in anteflection. Anteversion of pronounced degree may exist for years with but few if any symptoms. They are to a large extent due to the associated endometritis and metritis.
Vesical irritability is perhaps more common than in anteflexion. It is caused by the pressure of the fundus upon the bladder as well as by the associated cystitis.
Dysmenorrhoea and sterility are less common than in anteflexion. They may be caused by the close apposition of the external os to the posterior vaginal wall, though more probably by the chronic endometritis so commonly present. In those cases in which the fundus points downward and is on a lower level than the cervix, pain may be caused by the increased contractions necessary to expel the flow against the influence of gravity.
Menorrhagia, metrorrhagia and leucorrhoea are occasional symptoms, doubtless due to the accompanying congestion and endometritis.
Rectal symptoms are sometimes seen. An irritation, sometimes amounting to tenesmus, may result from the pressure of the cervix against the rectum. An obstructive constipation may result from the same cause.
Diagnosis
On digital examination the cervix is higher than normal. It is reached with difficulty and is directed backward toward the hollow of the sacrum. In extreme cases it may be directed somewhat upward. On passing the finger forward to the anterior vaginal vault the inferior surface of the body can be felt passing forward toward the symphysis. A careful bimanual examination should be made to confirm this position. The diagnosis is made from the extended position of the uterus, the cervix high, the fundus low, and the rigidity of the organ as a whole.
Treatment
This should begin with a removal of causes. These are most frequently inflammatory adhesions along the course of the sacro-uterine ligaments. The treatment of these differs in no way from the treatment of such adhesions described under anteflexion. The congestion, endometritis and metritis are treated by securing normal mobility for the uterus and by direct manipulation of the organ itself and to the tissues immediately surrounding it. The uterus can be bimanually replaced by passing two fingers of the right hand into the anterior formix of the vagina and lifting the fundus upward as far as possible at the same time an attempt is made by placing the fingers of the abdominal hand just above the symphysis, to approximate the fingers of the two hands in front of the fundus (Fig. 24). By this means the fundus is not only prevented from returning to its abnormal position, but can be pushed further backward and upward. The intravaginal fingers should now be placed in the posterior vaginal fornix and the cervix drawn downward and forward, the fundus being simultaneously pressed upward and backward with the abdominal hand (Fig. 25).
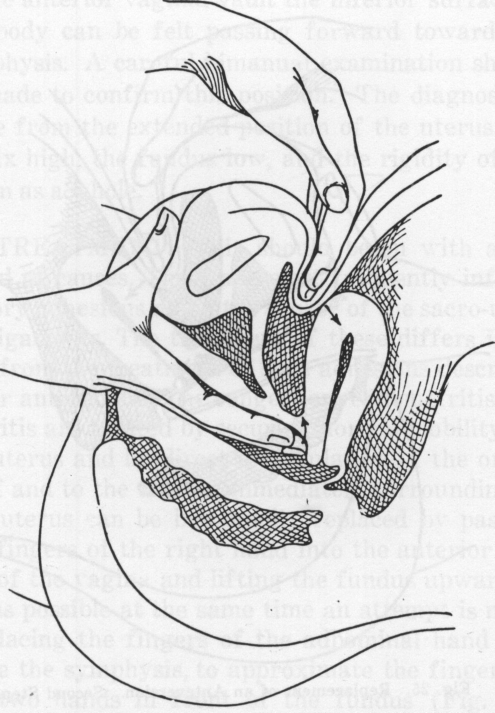
Fig. 24. Replacement of an Anteversion. First Step.
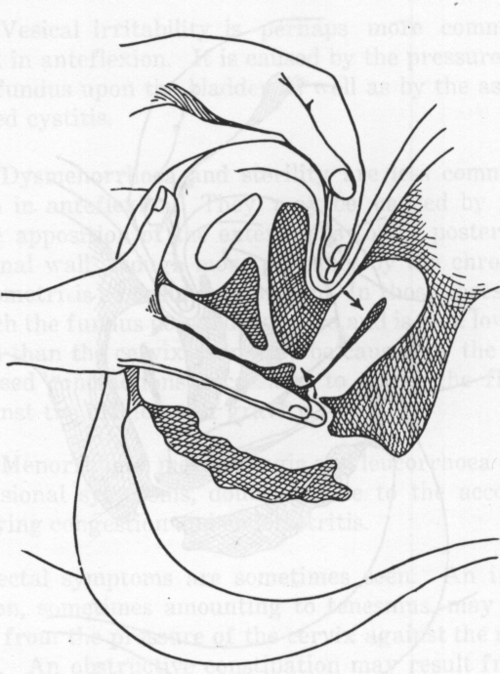
Fig. 25. Replacement of an Anteversion. Second Step.
This attempt at replacement should be made at every treatment, but it will not be permanently successful until the adhesions have been relaxed and the accompanying congestion or inflammation relieved.
The other causes are to be relieved by the usual methods.
Continue to:
My Books

