Pessaries. Part 2
Description
This section is from the book "Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs", by Percy H. Woodall, M. D., D.O.. Also available from Amazon: Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs.
Pessaries. Part 2
Pessaries support the tissues either directly or indirectly. In their turn they are supported by the pubic arch, the muscles and fasciae about the vaginal entrance, the vaginal wails and the pelvic floor. The pelvic floor when normal, through the medium of the intervening tissues, keeps the pessary held snugly against the pubic arch. Indirect support is by the so-called "lever action" in which the cervix is held backward and upward in the hollow of the sacrum (Fig. 68.) As before mentioned the uterus as a whole has a certain amount of normal rigidity because of which any elevation of the cervix tends to depress the fundus and vice versa. Thus, if the cervix be held upward and backward, the fundus must be downward and forward, unless the normal tissue rigidity has been overcome, as in cases of flexion. To maintain the cervix upward and backward is the purpose of the lever pessary. The posterior end of the pessary fits snugly into the posterior vaginal fornix, tensing the tissues here at their attachment to the cervix. The anterior end of the pessary gets its support primarily from the pubic arch and the pelvic floor. Unless the pelvic floor has been destroyed the vagina is more capacious within than at its opening. The narrow vaginal entrance aids in preventing the pessary from slipping out after it has been introduced.
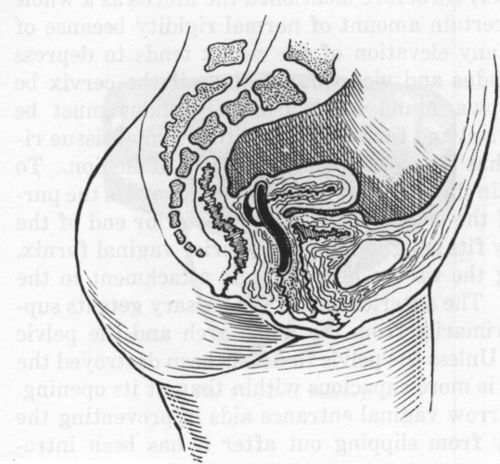
Fig. 68. Lever Action Pessary
Some direct support is exercised by every pessary but particularly is this so of the ring, the ball, and the belt pessaries in prolapsus.
It should always be remembered that pessaries must be "fitted" in the strictest meaning of that term. It is an easy matter to place a pessary in the vagina but unless it is properly fitted to the case it is either a useless contrivance, or on the other hand, may be the cause of irreparable harm. A pessary that is too small affords no support and is useless. One that is too large may by pressure cause inflammation, ulceration or perforation of the vaginal walls. A pessary should be so fitted and adjusted as to support the uterus in its normal position, to preserve its normal mobility and to restore to it, and not hinder, its normal circulation. To add to the difficulty of properly fitting a pessary is the fact that the contents of no two pelves are exactly alike. Vaginae differ in dimensions, in depth, in breadth, in capaciousness, in tonicity or relaxation of their walls. Uteri differ in size, in weight, in relation to the vagina and in their degree of displacement. The failure to properly appreciate these facts accounts for many of the unsatisfactory results in the use of pessaries. The correct fitting of a pessary is an operation that requires mechanical skill and a thorough knowledge of the contents of the pelvis and their possible variations. Especially is this true when a hard rubber "lever action" pessary is being used. It is nearly always necessary to reshape these instruments to fit the particular case.
Reshaping may be done by placing the pessary in hot water or by heating it over the flame of a spirit, or gas, lamp until it becomes pliable. It can now be reshaped by holding it with a towel and either lengthening, shortening, widening, narrowing or changing its curves as the indications may require. When the desired shape is secured the pessary is plunged into cold water which causes the new form to become permanent.
Pessaries may be used in practically all displacements, but are particularly useful in retrodisplacements and in prolapsus, not only of the uterus, but of the vaginal walls as well. In retroversion, during pregnancy and the puerperium, they are of distinct value. A retroverted uterus is prone to abortion and even though this does not occur, nausea and vomiting are more common when pregnancy occurs in such a uterus. In prolapse, pessaries are sometimes invaluable. In many cases it is a matter of choice between the use of a pessary and an operation. Operations are at times positively contra-indicated. I recall the case of a hemophiliac who refused to have a perineal laceration repaired but was restored to a condition of usefulness and comfort by the use of an inflated ring pessary. Also in cases of pregnancy with prolapsus they are of great usefulness.
Stem pessaries are sometimes successfully used in anteflexion, to straighten the cervical canal, and to relieve the accompanying dysmenorrhoea and sterility.
Elderly women in whom operations are extremely hazardous often secure great relief from the use of pessaries. In these, especial care must be taken to keep the instrument clean and to prevent incrustations upon it, because of the proneness of the thin vaginal walls of the aged to inflammation.
In complete prolapsus the belt pessary with supporting cords may be necessary. The vaginal walls themselves are thick and prolapsed; the pelvic outlet is relaxed, or destroyed, by a laceration and there is no support for any other form of pessary.
A pessary should be rendered surgically clean by scouring with soap and water, as a preparation for its introduction. It is then placed in an antiseptic solution and immediately preceding its introduction is well covered with a suitable lubricant.
In introducing the usual form of the modified ring pessary, that is those with a diameter longer antero-posteriorly than transversely, hold the anterior bar of the pessary with the thumb and index finger of the right hand and visualize its position and action when it is properly adjusted. Depress the perineum with the index finger of the left hand and introduce the posterior end of the pessary with its transverse diameter approximately in the direction of the vulval cleft, the bar of the pessary which is uppermost being kept to one side of the urethra to avoid painful pressure. After being introduced about half way the pessary is turned so that its transverse diameter lies horizontally with its posterior end di rected upward. It is now gently pushed backward until the posterior bar meets the resistance of the anterior surface of the cervix. The index finger of the right hand is now passed into the vagina beneath the pessary, the posterior bar is reached and disengaged from the front of the cervix and pushed behind it. The pessary is now in place and should be settled there by passing the index finger around it and gently lifting it upward and backward a few times. It should give neither pain nor discomfort when the patient gets upon her feet and walks about. In fact, if there is a consciousness of the presence of the pessary, it does not fit properly and it should be removed and either a smaller one, or one of another form, fitted.
A Hodge, a Thomas or a Smith pessary is most frequently used for retrodisplacements. While these appear very similar they each present some peculiarities that adapt them to different cases. Of these the Thomas pessary is most generally useful. Its broad posterior bar affords a larger surface for pressure and lessens the liability to erosion or ulceration. Its small anterior end fits well up under the symphysis and offers no interference with douching or copulation. Its decided curves from before backward offer good points of support by the tissues of the vaginal walls.
The Hodge pessary with its wider anterior bar will sometimes give better support if the floor of the pelvis is badly damaged. The broad posterior end of the Thomas pessary is sometimes too large to fit into the posterior fornix of the vagina, especially when the latter is small or shallow. The Smith pessary may be better adapted to this condition.
For prolapsus some form of the ring pessary is usually used. This pessary is primarily for support and has none of the lever action which is so essential in maintaining the uterus in its normal anteverted position. It merely raises and supports the uterus and the attached tissues. It is one form of pessary that may be used, and which may give a great deal of comfort, without the correction of the displacement. It secures its support by pressure against the vaginal walls and whatever muscles and fascia there may be remaining in the pelvic floor and about the vaginal outlet.
The simple ring pessaries are the flexible ring (made of coiled wire covered with rubber), the copper wire covered with rubber, the hard rubber ring and the soft rubber inflated ring. The latter is perhaps the most useful of these, but because of its broad surface, especial care is necessary to keep it clean and free of incrustations. It should be removed and thoroughly cleansed at least every week or ten days. Besides this a daily douche is necessary. After being worn for some time they may become deflated. They may be reinflated by means of a hypodermic syringe, the needle being inserted through a thickened spot that is easily found.
Both the elastic ring and the inflated ring pessaries have the advantage that they can be introduced in a partially compressed state. They then expand within the vagina.
Continue to:
My Books

