Backward Displacements. Part 3
Description
This section is from the book "Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs", by Percy H. Woodall, M. D., D.O.. Also available from Amazon: Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs.
Backward Displacements. Part 3
Treatment
Replacement of a retro-displaced uterus depends upon free mobility. Unless the uterus is freely moveable, replacement if effected is but temporary. A most careful bimanual examination must be made in every case to determine the cause of immobility, and the first indication in treatment is to remove such cause. Unfortunately this is not always possible.
Spinal innervation must be normalized. Inflammatory adhesions whether of connective tissue or peritoneal origin must be located and relaxed, as has been heretofore described. In some cases the uterus seemingly has to be "pried loose" from the anterior rectal or posterior pelvic wall, working downward with the abdominal hand and upward through the posterior vaginal vault or sometimes through the rectum with the intra-pelvic hand. (Fig. 32.)
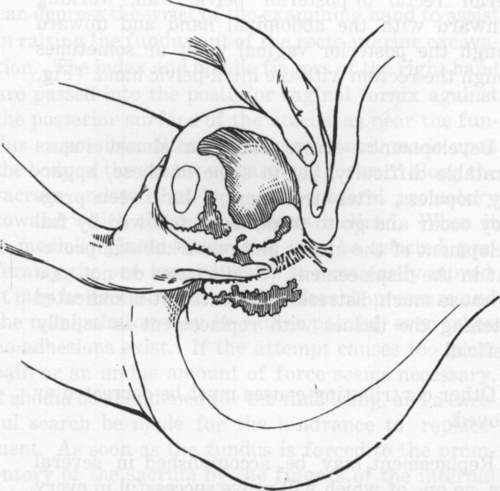
Fig. 32. Loosening the Uterus from the Posterior Pelvic Wall.
Developmental errors offer an almost insurmountable difficulty, yet in some of these, apparently hopeless, after treatment, I have seen pregnancy occur and go to term, to be followed by full development of the uterus and remarkable improvement in the displacement. Senile cases do not as a rule cause much distress. If treatment is indicated stretching the tissues with replacement is usually beneficial.
Other contributing causes must be corrected or removed.
Replacement may be accomplished in several ways, no one of which will prove successful in every case. Personally I have been most uniformly successful by using a bimanual abdomino-vaginal method, with the patient in the dorsal position, head and shoulders somewhat raised to relax the abdominal muscles. The bladder, rectum and pelvic colon should be empty. In these cases it in often best to have the patient brought to the end of the table so that, if necessary, you can not only stand between her knees and have the benefit of the weight of your body to press your fingers deeper into the pelvis, but can depress, the wrist of the examining hand to assist in raising the fundus out of the recto-uterine excavation. The index and middle fingers of the right hand are passed into the posterior vaginal fornix against the posterior surface of the uterus, as near the fundus as possible. Steady pressure is now made upon the body of the uterus upward and forward along the sacrum and to that side of the sacral promotory toward which the fundus seems inclined. When it is medially placed either side may be selected, preferably the one toward which it most easily moved. It may be necessary to use considerable pressure and the manipulation may be rather painful, even when no adhesions exist. If the attempt causes too great pain or an undue amount of force seems necessary, it should be abandoned for the time being, and a careful search be made for the hindrance to replacement. As soon as the fundus is forced to the promontory of the sacrum by the fingers of the internal hand, an attempt is made to get the heretofore idle fingers of the external hand behind the fundus from above by gentle, firm pressure upon the abdomen. In doing this place the hand upon the abdomen, press the superficial tissues upward so that they may be carried with the hand and it will not be necessary to move the hand over the skin. Now by downward
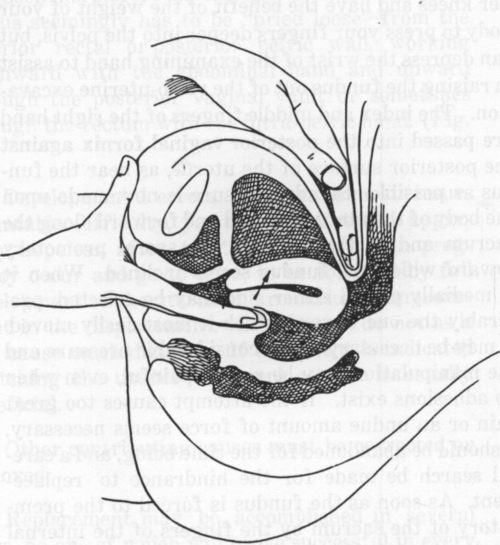
Fig. 33. Replacement of a Retroversion. First Step.
and backward vibratory pressure penetrate the pelvis from above and behind the fundus. The desire is to lift the fundus upward with the internal fingers and at the same time insinuate the external fingers behind it from above, and so approximate, as nearly as possible the fingers of the two hands and turn the fundus forward into its normal position. (Figs. 33, 34.) This is the most difficult part of the technic. The fingers of the operator may be too short, or the depth of the vagina may be insufficient to allow the fundus to be raised high enough, or the abdominal walls may be too thick or too contracted, to allow the external fingers to get sufficiently behind the fundus to turn it forward.
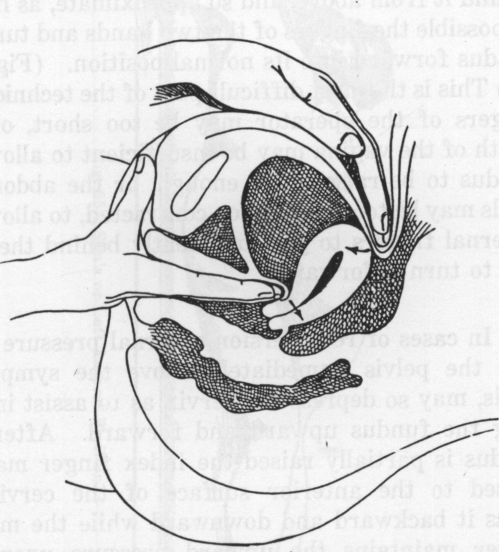
Fig. 34. Replacement of a Retroversion. Second Step.
In cases of retroversion external pressure deep into the pelvis immediately above the symphysis pubis, may so depress the cervix as to assist in tipping the fundus upward and forward. After the fundus is partially raised the index finger may be passed to the anterior surface of the cervix to press it backward and downward while the middle finger maintains the upward pressure upon the fundus so as to bring it in control of the external fingers. As soon as this is done the internal fingers are placed against the anterior part of the cervix and it is pushed backward and upward into the pelvis while the fundus is pressed downward and forward with the external hand. If the replacement is effected it is well to bring the uterus into a position of anteversion, and thus, as it were, over correct the displacement.
Occasionally better results may be obtained by lifting the fundus out of the recto-uterine excavation with the index or index and middle fingers introduced into the rectum.
An abdomino-recto-vaginal method is sometimes successful, the fundus being pushed upward by the index and middle fingers in the rectum while the cervix is forced backward by the thumb of the same hand in the vagina making pressure upon the anterior surface of the cervix. The abdominal hand lends the same assistance as before.
Again the Sims position (Fig. 35), or the knee-chest position may be used to advantage in dislodging the fundus from the depths of the pelvis. In either of these positions the index and middle fingers of the right hand are introduced into the posterior vaginal vault, the fundus is pushed upward and forward and while it is held in this position by the middle finger, the index finger is passed to the anterior surface of the cervix pushing it upward and backward.

Fig. 35. Sim's or Left Lateral Position.
Another method especially useful in retroflexion is to pass two fingers into the anterior vaginal vault and make backward pressure at the cervico-corporeal junction, or wherever the angle occurs, and straighten out the flexion angle by pressure against the sacrum. The uterus is now pressed upward in the direction of the sacro-iliac articulation; to the side of the promontory of the sacrum, and the fundus reached and pulled forward by the external hand as already described. (Fig. 36.)
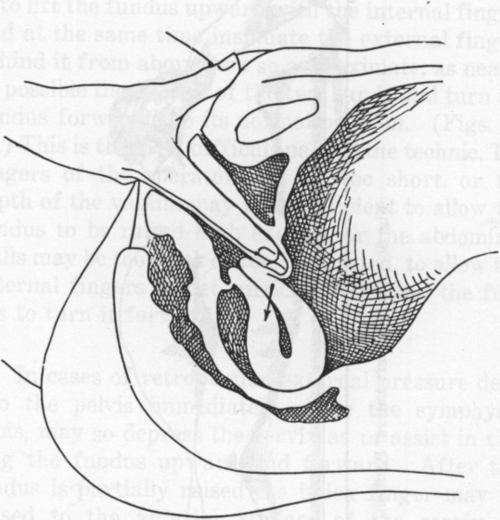
Fig. 36. Replacement of a Retroversion. Second Method.
Dr. C. W. Young secures splendid results in retro-displacements and in other intra-pelvic disorders by the use of the index finger in the vagina and middle finger in the rectum. The other hand is placed upon the abdomen giving an abdominovagina rectal manipulation. (Journal of the American Osteopathic Association, May, 1918.)
Whenever possible the patient should assume the knee-chest posture for several minutes after replacement, and then lie down in the Sim's position so that gravity will tend to prevent the uterus from resuming its mal-position. Instruct her to assume the knee chest posture for several minutes before retiring at night, and while in this posture have her separate the walls of the vagina so as to allow the entrance of air and thus balloon out its walls, securing the aid of atmospheric pressure as well as gravity in maintaining the proper position of the uterus. Other methods for maintaining proper position after it is once secured will be discussed in Chapter VIII (Tampons).
Continue to:
My Books

